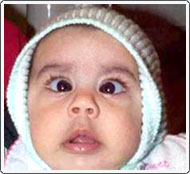
Very young child with very prominent congenital esotropia.

Patient is wearing a patch over the left eye to help force the use of the weaker right eye. The glasses are worn to correct the refractive error and improve vision while strengthening the right eye.
Key Points
- Onset within the first six months of life
- Infant uses either eye
- Usually associated with large-angle strabismus
- Best treated with early surgery
- Amblyopia in 50% of patients
- Poor prognosis for high-grade stereo acuity (depth perception)
Infantile esotropia, or congenital esotropia as it is often termed, is the most common form of infantile strabismus. It is defined as a large esotropia with onset prior to six months of age. The esotropia may present at birth although, in many cases, the esotropia is acquired during the first six months of life. Small intermittent exodeviations are common in normal infants, but esodeviations in newborns are rare. Persistent esotropia that is present after 2 months of age is probably pathologic and usually does not resolve spontaneously.
Patients may show strong fixation preference for one eye, which is an indication of amblyopia, or may alternate fixation (infant uses either to look at an object). Amblyopia occurs in approximately 50% of children with infantile esotropia. Esotropia in an infant may also be an important sign of vision loss. Disorders such as congenital cataracts and retinoblastoma often first present as infantile esotropia. No consistent inheritance pattern for infantile esotropia has been established, but it does tend to run in families. If any type of eye muscle problem runs in either side of the family, it would be a good idea to have the infant examined during the first 3 months of life to rule out any presence of crossed eyes (strabismus).
Treatment of Infantile Esotropia
In most cases, the treatment of infantile esotropia is surgical, usually operating on the medial rectus muscle in both eyes. In patients with farsightedness (hypermetropia of greater or equal to +3.00), spectacles should be prescribed first, as spectacles alone may correct the deviation. If amblyopia is present, it should be treated with patching prior to surgery.
Surgery for Infantile Esotropia
The standard approach has been to operate between 6 months and 2 years of age. This is based primarily on a study that showed that some fusion can be achieved if the eyes are aligned before 2 years of age. However, this fusion is subnormal binocular vision, and approximately half of the children with congenital esotropia will require multiple surgeries. Poor binocular fusion may be due to the fact that even brief periods of strabismus during the early period of visual development result in permanent loss of binocularity. More recently, Dr. Wright has shown that excellent fusion with high-grade stereopsis and good alignment can be obtained when surgery is performed prior to 6 months of age.
Surgery should be considered as early as 3 months of age if the following criterion are met:
- large-angle esotropia (40 prism diopters or more)
- constant or increasing deviation documented by 2 visits 1 month apart
- and the infant is a good anesthesia risk
